
Misdiagnosis is Real: Not All Heel Pain is Plantar Fasciitis
Apr 11, 2025Heel pain is one of the most common complaints in clinical practice. And let’s face it—“plantar fasciitis” often rolls off the tongue as the default diagnosis. But here’s the reality check: not all heel pain is plantar fasciitis, and misdiagnosis can lead to ineffective treatments, chronic pain, and frustrated patients.
The Problem with Assumptions
Many health professionals rely on pattern recognition:
Medial calcaneal pain + worse in the morning = plantar fasciitis.
While that might hold true in some cases, it’s a diagnostic shortcut that overlooks a wide spectrum of differential diagnoses. And if you're not clear on the source of the pain, the treatment can become a revolving door of trial and error.
Common Misdiagnoses That Mimic Plantar Fasciitis
Let’s unpack a few common culprits that can masquerade as “classic” plantar fasciitis:
-
🧠 Baxter’s Nerve Entrapment (Inferior Calcaneal Nerve)
Neuropathic pain, often sharp or burning, located more laterally or deep within the heel. It does not respond to stretching, orthotics, or typical fascial loading. -
🦶 Fat Pad Syndrome
Think “stone bruise.” Pain is often central to the heel, worsens on hard floors or barefoot walking, and may feel like walking on a pebble. -
🏃♂️ Calcaneal Stress Fracture
Usually in runners, military, or those with bone density issues. Pain increases with weight-bearing, and there may be swelling or pinpoint tenderness. -
🔗 Insertional Achilles Tendinopathy
Posterior heel pain, sometimes confused with plantar fascia because of close proximity. Look for stiffness during dorsiflexion (usually past 90 degrees) , triple flexion and load-based pain. -
⚡ Tarsal Tunnel Syndrome
Medial ankle/heel pain with burning, tingling, or radiating symptoms. Often misattributed to plantar fascia, especially when neural assessments are skipped.
The Cost of a Wrong Label
When plantar fasciitis is incorrectly diagnosed:
-
The patient may receive orthotics that worsen nerve entrapment.
-
They might be given load-based exercises that aggravate a fracture.
-
Fascial stretching could inflame a fat pad syndrome.
-
Or they’ll be left doing rehab that completely misses the actual cause of their symptoms.
Worse still, patients can become chronic pain cases, losing trust in both the clinician and the rehab process.
How to Assess the Differences: Neural vs Soft Tissue vs Bony Heel Pain
1. Listen to Language & Sensation
-
Burning, tingling, zapping, the client will flinch when pushing lightly over the area: Think nerve.
-
Bruised, dull, impact-sensitive: Think fat pad or bony.
-
Tight, pulling, stiff on first steps: Often fascial or tendinous.
2. Palpation Mapping
-
Medial tubercle tenderness? Likely plantar fascia.
-
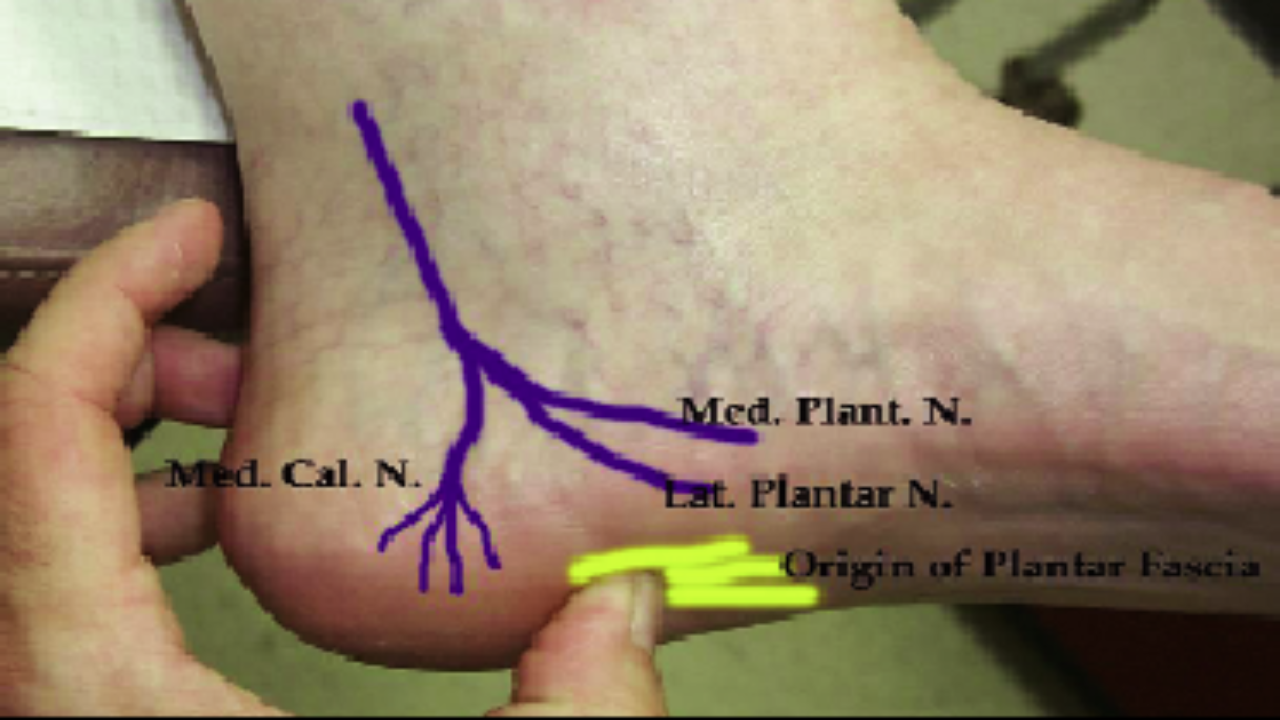
Lateral deep heel pain? Baxter’s nerve.
-
Posterior calcaneus? Achilles involvement.
-
Central heel with compression pain? Fat pad or fracture (quite rare) .
3. Neural Testing
-
Tinel’s sign over tarsal tunnel or along Baxter’s nerve path.
-
Sensory mapping and neural tension tests (e.g., SLR variations).
-
Ask about symptoms at rest or at night (often neural-related).
4. Load & Impact Testing
-
Jump tests or hopping—does this reproduce pain?
-
Gait analysis: Is the person avoiding heel strike?
-
Single-leg stance and slow-motion dorsiflexion—observe movement control.
5. Imaging When Needed
-
Ultrasound can help with fascial thickening or inflammation, (although most will have this, so it is not acurate))
-
MRI or bone scan for suspected stress fractures.
-
Diagnostic ultrasound for entrapments.
Reframing Heel Pain for Better Outcomes
By moving beyond the "plantar fasciitis" label, we open the door to:
-
More accurate treatment plans
-
Better patient buy-in
-
Faster, more effective recovery outcomes
And crucially: it positions you as a clinician who understands complexity.
When you factor in fascial anatomy, nerve entrapments, kinetic chain influences, and proper loading principles, you begin to see the foot as part of a larger system—not just a localised pain generator.
✅ Conclusion: A Better Diagnostic Process Starts at the Heel
The next time a patient presents with heel pain, don’t default to plantar fasciitis.
Instead:
-
Think systemically, not symptomatically.
-
Be curious, not assumptive.
-
Test broadly, treat specifically.
Heel pain is complex, but misdiagnosis doesn’t have to be part of the story. With better assessment tools and a wider diagnostic lens, you can become the clinician who turns persistent pain cases into solved ones.
